
Surgical aortic valve alternative (SAVR) prolongs life and improves its high quality in sufferers with extreme aortic stenosis (AS). Unplanned SAVR is a failure of AS screening and follow-up programmes. We recognized all elective, first, remoted SAVRs carried out between 1 January and 31 December 2019 in a Welsh tertiary cardiac centre, and documented the scientific and echocardiographic variables, and causes for unplanned SAVR.
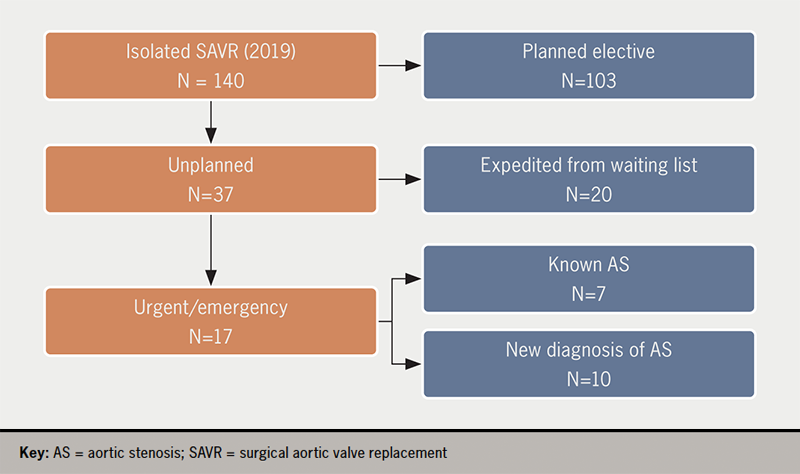
Of 140 remoted SAVR, 37 (26%) have been unplanned (16 feminine, imply age 72.3 ± 8.4 years). Twenty had been on the SAVR ready checklist and had expedited operations due to considerations in regards to the severity of the AS (12 sufferers), or due to acute (4 sufferers) or power (4 sufferers) left ventricular failure (LVF). Of the 17 not on the ready checklist, AS was identified in seven: three had acute pulmonary oedema whereas below follow-up with ‘reasonable AS’, one had been referred however developed pulmonary oedema whereas ready for a surgical outpatient appointment, one refused SAVR however was subsequently admitted with acute pulmonary oedema and accepted SAVR, one was admitted instantly from house as a result of considerations about worsening AS, and one had infective endocarditis with extreme aortic regurgitation. Of 10 sufferers with a brand new analysis of AS, 5 offered with LVF, 4 with angina and in three there was a historical past of syncope (p=0.003 vs. identified AS; a number of signs). Survival, age, Canadian Cardiovascular Society (CCS) and New York Coronary heart Affiliation (NYHA) class, variety of danger elements, peak and imply aortic valve (AV) gradients, AV space, and stroke quantity index weren’t completely different between sufferers who had deliberate versus unplanned SAVR, or with identified or new AS. Sufferers with a brand new analysis of AS had longer pre-operative wait (22.3 ± 9.3 vs. 6.0 ± 10.3 days, p<0.001).
In conclusion, 1 / 4 of SAVRs are unplanned and half are in sufferers and not using a prior analysis of AS. Unplanned SAVR is related to extended size of hospital keep and with a historical past of syncope, however different typical scientific and echocardiographic parameters don’t differ between sufferers present process deliberate versus unplanned SAVR.
Introduction
Surgical aortic valve alternative (SAVR) is the perfect established remedy for extreme, symptomatic aortic valve stenosis (AS), the place it restores life-expectancy to ranges seen within the common inhabitants.1 Ideally, sufferers with AS must be followed-up in a valve clinic, in order that the optimum timing for performing SAVR might be decided, primarily based on a mixture of periodically assessed signs, indicators, imaging and laboratory exams.2,3 Working too late carries an elevated danger of demise and of peri-operative issues, associated to (doubtlessly irreversible) deterioration of left ventricular (LV) perform from afterload mismatch.4
From this angle, any occasion of SAVR carried out as an unplanned process is a missed alternative to offer well timed care with the minimal potential danger.
We got down to analyse pressing, unplanned SAVR procedures in our centre, in an effort to grasp elements that specify why some sufferers ‘slip by means of the web’ and are operated on in an unplanned method, to assist us decide what might be completed to keep away from this sooner or later.
Technique
Setting
Morriston cardiac centre supplies tertiary cardiology and cardiac surgical care to a inhabitants of about a million in West Wales, UK; there are 5 cardiac surgeons working in two cardiac theatres, performing roughly 750 open-heart procedures yearly.
Inclusion and exclusion standards
We chosen all unplanned (pressing or emergency) remoted, first SAVR procedures carried out for AS in 2019, the final full 12 months earlier than the COVID-19 pandemic. We excluded SAVRs that had related procedures, corresponding to coronary artery bypass graft (CABG), root alternative, or concomitant intervention of any sort for an additional coronary heart valve pathology.
Knowledge evaluation
The urgency of the operation was ascertained from our digital surgical database (Dendrite Medical, Studying, UK). We additionally used the Welsh Medical Portal to doc patient- and procedure-related variables, in addition to the pathway every affected person {followed} between analysis and pressing/emergency SAVR, with the intention to determine elements that will have led to unplanned SAVR. Particularly, we documented presence and severity of AS signs on admission, whether or not sufferers have been on a ready checklist for SAVR on the time of their unplanned operation, whether or not the analysis of AS pre-dated the admission or not, which of the most important cardiovascular danger elements have been current, echocardiographic descriptors of the severity of the AS (peak aortic velocity, imply aortic gradient, aortic valve space by continuity, stroke quantity index) and LV ejection fraction (LVEF) on the transthoracic echo closest to the date of SAVR, stage of AS-related myocardial harm,5 time lag between admission and operation, and the size of complete and of postoperative hospital keep, in addition to survival standing (with a censoring date of 21 December 2021). We in contrast scientific and echo parameters between sufferers on, and people not on, the SAVR ready checklist, and between sufferers with identified AS versus these with a brand new analysis of AS throughout the index admission, utilizing the Chi-square statistic for nominal variables and Pupil’s t statistic for ordinal, steady variables; p<0.05 was deemed vital. The place the belief of equal variance was violated we used the Welch and Mann-Whitney exams. We used JASP 0.16.0.0, an open-source statistical package deal, (https://jasp-stats.org/) for the statistical evaluation.
Outcomes
Sufferers
In 2019 there have been 103 elective, first-time, remoted SAVRs and 37 (16 feminine, imply age 72.3 ± 8.4 years) non-elective, remoted, first SAVR (26% of complete 140 SAVRs). Of those, 20 sufferers have been already on the ready checklist for SAVR and 17 weren’t (determine 1).
Medical traits
Medical traits of the sufferers are summarised in desk 1, which is assessed by sufferers on the ready checklist versus sufferers not on the ready checklist, and sufferers with a pre-existing analysis of AS versus sufferers with out such a analysis. Frequency and severity of angina and of coronary heart failure, prevalence of danger elements (desk 2), aortic valve space, imply gradient and peak velocity, in addition to stroke quantity index and LVEF, weren’t completely different between those that have been on the ready checklist for SAVR, in contrast with those that weren’t, though LVEF was numerically decrease and imply gradient numerically larger in sufferers who weren’t on the ready checklist. The identical findings apply to affected person teams outlined by whether or not a analysis of AS was identified earlier than the index admission. Virtually one in three sufferers and not using a pre-existing analysis of AS offered with syncope, a a lot larger proportion than in these with identified AS, however the significance of this discovering is unsure given the small measurement of our pattern.
Desk 1. Medical and echocardiographic traits of sufferers stratified in accordance with whether or not they have been on the surgical ready checklist for surgical aortic valve alternative (SAVR) or not, and whether or not they had been identified with aortic stenosis (AS) or not previous to the index admission for SAVR. Variables in daring achieved statistical significance for the distinction between the teams
Variable, imply ± SD
Not on W/L for SAVR
On W/L for SAVR
p
AS not identified
Identified AS
p
Age at admission, years
72.4 ± 8.7
72.2 ± 8.3
0.98
72.8 ± 9.1
72.1 ± 8.3
0.84
CCS angina class
1.6 ± 0.9
1.6 ± 0.8
0.87
1.4 ± 0.7
2.7 ± 0.8
0.04
NYHA coronary heart failure class
2.8 ± 0.9
2.6 ± 0.7
0.40
2.7 ± 0.9
2.7 ± 0.8
0.80
Variety of cardiac danger elements
1.7 ± 0.8
1.8 ± 1.1
0.80
1.9 ± 0.7
1.7 ± 1.1
0.75
Peak velocity throughout AV, m/s
4.5 ± 0.8
4.1 ± 0.9
0.18
4.5 ± 0.8
4.1 ± 0.9
0.31
Imply aortic valve gradient, mmHg
50.1 ± 20.0
40.8 ± 19.3
0.15
50.5 ± 19.7
43.1 ± 20.0
0.31
Aortic valve space, cm2
0.6 ± 0.2
0.6 ± 0.1
0.55*
0.6 ± 0.2
0.6 ± 0.1
0.43
LV ejection fraction, %
49.4 ± 13.3
54.2 ± 10.3
0.22
52.2 ± 11.3
51.9 ± 12.3
0.95
Stroke quantity index,ml/m2
34.5 ± 7.6
33.2 ± 8.2
0.61
33.4 ± 7.7
33.9 ± 8.0
0.87
Pre-operative hospital keep, days
20.0 ± 11.8
2.2 ± 4.3
0.001*
22.3 ± 9.3
6.0 ± 10.3
0.001
Postoperative hospital keep, days
16.4 ± 16.2
9.4 ± 6.7
0.008
12.5 ± 10.0
12.7 ± 3.3
0.9
Whole hospital keep, days
36.5 ± 21.9
11.7 ± 7.7
0.01*
34.8 ± 13.9
18.77 ± 20.4
0.029
*Levene’s take a look at was vital (p<0.05), suggesting a violation of the equal variance assumption, however p values remained the identical with Welch’s and Mann-Whitney’s exams.Key: AS = aortic stenosis; AV = aortic valve; CCS = Canadian Cardiac Society; LV = left ventricle; NYHA = New York Coronary heart Affiliation; SAVR = surgical aortic valve alternative; SD = normal deviation; W/L = ready checklist
Desk 2. Distribution by gender, principal symptom at presentation and cardiovascular danger elements in accordance with whether or not sufferers have been on the ready checklist for SAVR or not and whether or not sufferers have been identified with AS earlier than presentation or not
Affected person traits and signs
Not on W/L for SAVR
On W/L for SAVR
p
AS not identified
Identified AS
p
Gender
F
9
7
0.27
5
11
0.60
M
8
13
5
16
Angina
No
12
16
0.50
6
22
0.17
Sure
5
4
4
5
Coronary heart failure
No
8
6
0.28
6
8
0.09
Sure
9
14
4
19
Syncope
No
14
20
0.05
7
27
0.03
Sure
3
0
3
0
T2DM
No
12
12
0.50
8
16
0.24
Sure
5
8
2
11
Excessive BP
No
7
7
0.62
2
12
0.62
Sure
10
13
8
14
Present smoking
No
15
20
0.11
9
26
0.45
Sure
2
0
1
1
Household historical past of CAD
No
16
17
0.3
10
23
0.3
Sure
1
3
0
4
Power renal illness
No
14
18
0.4
9
23
0.70
Sure
3
2
1
4
Key: AS = aortic stenosis; BP = blood stress; CAD = coronary artery illness; SAVR = surgical aortic valve alternative; T2DM = kind 2 diabetes mellitus; W/L = ready checklist
Size of hospital keep
Size of hospital keep was considerably longer in sufferers who weren’t on the ready checklist: complete size of keep (imply of 36.5 ± 21.9 days vs. 11.7 ± 7.7 days, p<0.01); pre- and post-operative size of keep was additionally longer in sufferers not on the ready checklist (desk 1). Findings have been comparable for a comparability between sufferers with, versus these with out, a pre-existing analysis of AS (desk 1).
Affected person pathways to SAVR
Sufferers with a earlier analysis of AS
There have been 27 sufferers with identified AS. Of those, 20 have been on the ready checklist and 7 weren’t. Causes resulting in expedited SAVR within the 20 sufferers on the ready checklist included concern about how extreme the AS was (12 sufferers – operation introduced ahead by the surgeon, after the preliminary surgical clinic appointment), and the event of a scientific emergency in eight: 4 instances of acute pulmonary oedema and 4 instances of congestive coronary heart failure. Of seven sufferers not on the ready checklist, three had acute pulmonary oedema whereas below routine cardiology follow-up for ‘reasonable AS’, one had been referred however developed pulmonary oedema whereas ready for a surgical outpatient appointment, one refused SAVR however was subsequently admitted with acute pulmonary oedema, one was admitted instantly from house due to considerations from the GP in regards to the severity of AS, and one had infective endocarditis on a background of gentle AS, and was admitted with extreme acute aortic regurgitation.
Sufferers and not using a earlier analysis of AS
In 10 sufferers the analysis of AS was first established throughout the admission that led to SAVR: 5 offered with LV failure, 4 with angina and in three there was a historical past of syncope (p=0.003 vs. identified AS; complete >10 as some sufferers had a number of signs).
Desk 3. Survival standing in accordance with whether or not sufferers have been on the ready checklist or not, and to whether or not they had been identified with AS earlier than the index admission
Not on W/L for SAVR
On W/L for SAVR
p
AS not identified
Identified AS
p
Alive
15
16
0.49
9
22
0.53
Useless
2
4
1
5
Key: AS = aortic stenosis; SAVR = surgical aortic valve alternative; W/L = ready checklist
Desk 4. Time between preliminary analysis of AS and SAVR in years and the variety of sufferers with and and not using a prior analysis of AS, in accordance with whether or not sufferers have been on the ready checklist or not
Not on W/L for SAVR
On W/L for SAVR
Time between preliminary analysis of AS and SAVR in years (p=0.49)
N
17
20
Imply ± SD
1.8 ± 2.3
2.4 ± 2.3
Minimal
0.0
0.2
Most
5.8
8.9
Prior analysis of AS (p<0.001)
No
10
0
Sure
7
20
Whole
17
20
Key: AS = aortic stenosis; SAVR = surgical aortic valve alternative; SD = normal deviation; W/L = ready checklist
Each sufferers not on the ready checklist and people with a brand new analysis of AS had numerically worse indices of AS, however the variations weren’t vital. There was no distinction in mortality, or within the stage of AS-related myocardial harm at presentation between sufferers on, or not on, the ready checklist, or these with a previous versus a brand new analysis of AS (tables 3, 4 and 5). The extent of AS-related myocardial harm was not completely different between survivors and deceased (desk 5).
Dialogue
In a tertiary UK cardiac centre serving a inhabitants of 1 million, 12% of SAVR (17 of 140) have been pressing, unplanned, and had elevated pre-operative size of hospital keep. Virtually half of those (7/17, 44%) unplanned SAVRs have been in sufferers and not using a earlier analysis of AS.
One other 20 operations (14% of SAVR) have been expedited from the ready checklist. These have been sufferers who had been accepted for SAVR, however whose operations have been introduced ahead by surgeons involved in regards to the severity of the illness, or who decompensated with coronary heart failure whereas ready for his or her process. For service enchancment, learning sufferers who had unplanned operations is prone to be most informative.
Sufferers with operations expedited whereas on the ready checklist for SAVR
Sufferers on the ready checklist for SAVR have had pre-operative investigations accomplished and, in precept, might obtain their SAVR at any time after they’ve been positioned on the ready checklist. If the NHS had the capability to carry out well timed operations, this class of sufferers wouldn’t exist, or their quantity could be negligible. Restricted capability signifies that – unavoidably – some sufferers will decompensate whereas ready for elective SAVR.
Desk 5. Stage of myocardial harm by whether or not sufferers have been on the ready checklist for SAVR, had identified AS, and mortality
Stage of myocardial harm
Not on W/L for SAVR
On W/L for SAVR
AS not identified
Identified AS
Alive
Useless
0
3
2
2
3
5
0
1
4
2
7
9
11
0
2
6
9
4
11
11
4
3
4
1
2
3
3
2
4
0
1
0
1
1
0
Whole (N=37)
17
20
10
27
31
6
p worth
0.37
0.79
0.16
Key: AS = aortic stenosis; SAVR = surgical aortic valve alternative; W/L = ready checklist
In our pattern of 37 sufferers, 20 have been recognized by their physicians as needing an expedited operation, and thus they ‘jumped the queue’ to an early SAVR, which is a compromise answer for the supply of efficient care inside a constrained sources setting. Broadly talking, these sufferers might be thought of a ‘surrogate’ for the bigger group of sufferers having genuinely elective, deliberate procedures, which don’t must be introduced ahead. Nevertheless, of those 20, solely 12 have been clinically steady and had expedited surgical procedure due to considerations in regards to the severity of the AS, whereas the opposite eight had developed coronary heart failure that prompted early surgical procedure. Though current guidelines6 nonetheless emphasise presence of signs as an vital set off for SAVR, coronary heart failure (or any signs) in AS is an ‘end-stage’ manifestation with a dire outlook in a situation with an extended asymptomatic part. Nevertheless, the tide could also be about to show, with current proof from randomised-controlled trials that early surgical procedure is related to markedly improved survival in asymptomatic sufferers with very severe7 or extreme asymptomatic AS,8 when put next with typical, guideline-driven observe. In mild of those newest information, having sufferers develop coronary heart failure after they’ve already been accepted for SAVR will grow to be an untenable proposition.
Sufferers with AS not on the ready checklist for SAVR
All seven such sufferers have been below yearly cardiology follow-up with a analysis of ‘reasonable aortic stenosis’, and three had been seen in a cardiology or valve clinic inside three months of the index admission. The one distinction we might determine was an extended complete, pre- and postoperative hospital keep in contrast with sufferers who have been on the ready checklist (desk 1). Sufferers on this group had numerically extra extreme indices of AS, and decrease LVEF, suggesting extra superior illness, however the variations weren’t vital, presumably because of the low numbers concerned. Clearly, the follow-up delivered by our valve clinics is imperfect, having didn’t predict decompensation, albeit in a small variety of sufferers. Potential causes stay speculative because of the small measurement of the group, however could embody underestimation of AS severity (though the upper gradients noticed would determine these as instances of genuinely extreme AS), reluctance of the valve clinic to refer for SAVR for scientific causes (though the truth that sufferers ended up having SAVR mitigates in opposition to such a chance) or under-reporting of signs by stoical sufferers. Whether or not a wider use of N-terminal proB-type naturietic peptide (NT-proBNP) ranges and of aortic valve calcium scoring by computed tomography (CT)6 for monitoring AS development can stop such ‘near-misses’ stays to be seen.
Sufferers with AS not identified till the index admission
The ten sufferers on this class had a life-threatening complication of their valve illness as its first manifestation. No enchancment within the effectivity of our present mannequin of look after sufferers with AS would scale back this proportion; to realize that, lively screening for AS could be wanted. In a earlier research from the identical geographic space, we discovered a prevalence of 8% of at the very least reasonable mitral regurgitation (MR), and 5% of at the very least reasonable AS (complete prevalence 13%) in asymptomatic folks over the age of 75,9 barely larger than in the same Ox-Valve research, which discovered a complete inhabitants prevalence of reasonable or extreme valvular coronary heart illness (VHD) of 11.3% in barely youthful topics.10 The fee/profit implications of such an strategy want additional research, however a main care-based population-screening programme could turn into cost-effective and clinically possible by doubtlessly avoiding the lengthy hospital stays related to SAVR in sufferers with beforehand undetected AS.
Size of hospital keep (LOHS)
Constantly, sufferers with the least diploma of planning of their SAVR (these with identified AS however not on the ready checklist, and people and not using a earlier analysis of AS) spent longer in hospital than both these on the ready checklist or these with a earlier analysis of AS. The variations within the size of the pre-operative keep have been most placing between sufferers on, versus these not on, the ready checklist, with a imply of two.2 ± 4.3 versus 20.0 ±11.8 days (p<0.001) (desk 1), and have been much less marked for the postoperative keep. Sufferers with out, versus these with, a analysis of AS had a imply pre-operative hospital keep of twenty-two.3 ± 9.3 versus 6.0 ± 10.3 days (p<0.001), whereas the postoperative keep was not completely different. Our information will not be granular sufficient to permit us to grasp the precise causes of those variations, however they’re prone to be a composite of delays regarding the provision of a mattress to permit switch from the admitting hospital to the surgical centre, and of the time it takes to stabilise and examine acutely unwell sufferers.
Paradoxically, the discovering of vastly longer LOHS in sufferers present process expedited or unplanned SAVR could also be crucial motivator for enhancing the method of detection and monitoring of AS within the NHS. Additional analysis is required with the intention to mannequin the web impact on healthcare prices of a screening programme for coronary heart valve illness in the neighborhood.
Referral to remedy time (RTT)
The RTT for remoted SAVR in our hospital throughout the research interval was 25 weeks. The importance of our findings is evidently depending on the broader context of the healthcare system: sufferers who have been already on the ready checklist wouldn’t have needed to current in extremis if the valve intervention might have been delivered sooner after analysis. Furthermore, the goalposts are transferring on a regular basis, with the provision of transcatheter aortic valve alternative (TAVR) now lowering ready checklist time to weeks after the analysis is made and the indication for valve intervention established.
Limitations
Dimension of the research
It is a small research, because it was designed and carried out by busy clinicians reasonably than by devoted analysis employees, and, as such, doubtlessly vital variations between the assorted subgroups could not have reached the importance threshold. Nevertheless, regardless of the low numbers, it affords an correct ‘snapshot’ of the affected person journey in a system with restricted sources. We didn’t have the sources to gather detailed information on sufferers who had genuinely elective procedures, however our class of ‘expedited SAVR’ is prone to be broadly equal to these.
Evaluation of myocardial harm
A limitation of our research is that imaging markers of myocardial harm, corresponding to T1 mapping or late gadolinium enhancement (LGE) by cardiac magnetic resonance (CMR), weren’t out there; such markers could enable additional danger stratification of sufferers being followed-up for AS.
Relevance of SAVR within the TAVR period
The appearance of percutaneous aortic valve alternative has modified the panorama of valve intervention past recognition,11 and the indications are increasing quickly to embody low-risk sufferers.12 It’s probably that we will see an additional diminution of the proportion of sufferers present process SAVR, simultaneous to a significant enhance within the complete variety of aortic valve interventions, with open surgical procedure reserved sooner or later for sufferers with concomitant pathologies, corresponding to coronary artery illness not appropriate for percutaneous coronary intervention (PCI) or aortic illness in want of surgical remedy. The proportion of sufferers for whom our findings are related will most likely diminish, however SAVR is unlikely to grow to be extinct, and the sturdiness of TAVR valves continues to be not totally established, so our findings can nonetheless generate helpful impetus for service enchancment.
Conclusion
With the present mannequin of care within the NHS, a major proportion of sufferers have SAVR, the life-saving remedy for AS, carried out in an unplanned method, precipitated by scientific decompensation; such sufferers have the next incidence of syncope. Unplanned surgical procedure results in extended hospital keep, an undesirable final result. A small proportion of the unplanned operations are carried out in sufferers and not using a prior analysis of AS; such sufferers might solely be detected by rolling out a screening programme for coronary heart valve illness in the neighborhood.
Key messages
Intervening in instances of aortic stenosis requires a programme of shut surveillance of the sufferers’ symptomatology, echocardiographic parameters and suitability for modern aortic valve alternative procedures
Whereas surgical aortic valve alternative in an acceptable candidate affords unmatched outcomes by way of sturdiness, performing this process in an expedited or unplanned style could result in pointless morbidity by way of size of hospital keep
In a resource-limited public well being programme, valvular screening programmes must be enhanced to select instances of silent valvular degeneration and facilitate well timed intervention of progressive aortic valve illness
Conflicts of curiosity
None declared.
Funding
None.
Examine approval
Requirement for moral approval and consent was waived by the native hospital audit division because the research is a retrospective evaluation of anonymised affected person information.
References
1. Vahanian A, Beyersdorf F, Praz F et al. 2021 ESC/EACTS pointers for the administration of valvular coronary heart illness. EuroIntervention 2022;17:e1126–e1196. https://doi.org/10.4244/EIJ-E-21-00009
2. Chambers JB. run a specialist valve clinic: the historical past, examination and train take a look at. Echo Res Pract 2019;6:T23–T28. https://doi.org/10.1530/ERP-19-0003
3. Chambers JB, Parkin D, Rimington H et al. Specialist valve clinic in a cardiac centre: 10-year expertise. Open Coronary heart 2020;7:e001262. https://doi.org/10.1136/openhrt-2020-001262
4. Ross J. Afterload mismatch in aortic and mitral valve illness: implications for surgical remedy. J Am Coll Cardiol 1985;4:811–26. https://doi.org/10.1016/S0735-1097(85)80418-6
5. Vollema EM, Amanullah MR, Ng ACT et al. Staging cardiac harm in sufferers with symptomatic aortic valve stenosis. J Am Coll Cardiol 2019;74:538–49. https://doi.org/10.1016/j.jacc.2019.05.048
6. Otto CM, Nishimura RA, Bonow RO et al. 2020 ACC/AHA guideline for the administration of sufferers with valvular coronary heart illness: government abstract. A report of the American School of Cardiology/American Coronary heart Affiliation Joint Committee on Medical Follow Pointers. Circulation 2021;143:e35–e71. https://doi.org/10.1161/CIR.0000000000000932
7. Kang DH, Park SJ, Lee SA et al. Early surgical procedure or conservative look after asymptomatic aortic stenosis. N Engl J Med 2020;382:111–19. https://doi.org/10.1056/NEJMoa1912846
8. Banovic M, Putnik S, Penicka M et al. Aortic valve alternative versus conservative remedy in asymptomatic extreme aortic stenosis: the AVATAR trial. Circulation 2022;145:648–58. https://doi.org/10.1161/CIRCULATIONAHA.121.057639
9. Williams C, Mateescu A, Rees E et al. Level-of-care echocardiographic screening for left-sided valve coronary heart illness: excessive yield and inexpensive price in an aged cohort recruited in main observe. Echo Res Pract 2019;6:71–9. https://doi.org/10.1530/ERP-19-0011
10. d’Arcy JL, Coffey S, Loudon MA et al. Giant-scale neighborhood echocardiographic screening reveals a significant burden of undiagnosed valvular coronary heart illness in older folks: the Ox-VALVE inhabitants cohort research. Eur Coronary heart J 2016;37:3515–22. https://doi.org/10.1093/eurheartj/ehw229
11. Arora S, Misenheimer J, Ramaraj R. Transcatheter aortic valve alternative: complete overview and current standing. Tex Coronary heart Inst J 2017;44:29–38. https://doi.org/10.14503/THIJ-16-5852
12. Spears J, Al-Saiegh Y, Goldberg D, Manthey S, Goldberg S. TAVR: a overview of present practices and issues in low-risk sufferers. J Interv Cardiol 2020;2020:2582938. https://doi.org/10.1155/2020/2582938











{kind=link}