
Andreas Grüntzig, an ardent angiologist crafted an indeflatable sausage-shaped dual-lumen balloon-catheter, designed its supply to the center, launched minimally invasive coronary intervention and taught by beaming dwell demonstration. Subsequent advances are simply incremental tweaks and tinkers round this totally fashioned framework from 1978. The near-immediate or immediate suggestions studying course of by which the center responds to any new invasive procedural variation facilitates every new change; be it drug-eluting stent, drug-coated balloon, or each in numerous combos and permutations. Now with Grüntzig’s balloon armed with an antiproliferative drug, it may dominate the sphere as soon as extra, as he initially envisaged.
Introduction
Using drug-coated balloon (DCB) in de novo coronary artery illness has seeped by means of into routine follow in recent times.1 Largely unnoticed by the mainstream group, ignored by multi-national machine firms and infrequently mentioned at worldwide conferences. Its improvement truly parallels that of first-generation drug-eluting stent (DES) from the early 2000s; pioneered, propagated and instructed by skilled German operators.2,3 Its efficacy is confirmed for in-stent re-stenosis (ISR),4 small vessel illness,5,6 high-risk bleeder,7 and the place stenting is perhaps prevented, corresponding to in Takayasu arteritis.8 It has been safely trialled in ST-elevation myocardial infarction (STEMI),9,10 side-branch involving left foremost,11–13 multi-vessel,14 large-vessel15 and calcified16,17 illness. Merely put, the entire spectrum of ischaemic coronary heart illness is amenable to DCB, however ectatic or aneurysmal coronary lesion that’s too massive to stent.18,19
DCB follow
Looking out with the phrases “DCB”, “coronary” and “de novo” in Google Scholar brings up publications reaching 100 per thirty days in 2022, in contrast with 140 for DES. Though the present drive for DCB is principally in Far Japanese and Nordic international locations. Nevertheless, the evidence-base and strut/polymer/drug know-how for DES have matured and its worth has been pushed down by competitors. DCB prices two to 3 occasions greater than DES. With the realisation that the majority of coronary interventions could possibly be accomplished with DCB, it’s conceivable that huge gamers will quickly enter the foray. Cordis Company, which implanted the primary DES in 1999 and launched it in 2003, has simply reportedly acquired a DCB being studied for de novo use for practically £1 billion. Its first-generation DES was hamstrung by thick stent strut, polymer allergy, stent thrombosis and extra mortality after two years.20 It would lead once more, utilizing the identical antiproliferative drug, this time delivered not with stent, however by balloon. Therefore, leaving nothing behind, that’s, no stent, no stent thrombosis.
In 2022 alone, over a million DCB-only or 20–25% of coronary interventions had been undertaken in China. Within the UK, DCB use was 8.1%, primarily for ISR however with a small de novo part, in keeping with the British Cardiovascular Intervention Society (BCIS) nationwide audit knowledge from 2021/2022. If 70% of coronary instances are accomplished with DCB within the UK, it might be an estimated £30 million market each year within the subsequent 5 to 10 years (see under for DCB vs. DES cut up). The DCB journey is akin to that of radial method adoption, which is presently the dominant vascular entry by diktat following a 25-year journey from fringe to the forefront. Every method has its personal efficiency bias. With radial entry, the mortality profit in acute coronary syndrome is just obvious within the above 70% high-volume operators.21,22 DCB is comparable, and its quarter-century voyage reaches its zenith by 2028, as coronary intervention did in 2003, when the creator began his coaching.23
The start
Percutaneous coronary transluminal angioplasty or plain-old balloon angioplasty (POBA) was first reported in The Lancet by Andreas Grüntzig (1939–85), a visionary German angiologist.24 He improved on Charles Dotter’s method performing peripheral angioplasty together with his patented double-lumen balloon-catheter. He cast his sausage-shaped balloon with polyvinyl chloride (PVC) plastic after consulting with Heinrich Hopff, a retired German natural chemist in Zurich.25 He designed a system with pressured-and-contrasted balloon indeflation, blood stress transducing and radiographic-dye injection for visualization to carry out coronary angioplasty. This was with low-resolution cine-fluoroscopy with out the replay button. He first examined his balloon on canines, adopted by sufferers present process coronary artery bypass grafting (CABG). It was a theatrical efficiency then, as it’s immediately, when he imparted his method broadcasted to a dwell viewers beginning on 7–10 August 1978; 4 such conferences occurred in Zurich whereas he was there.25–27
POBA has an immediate suggestions for fulfillment or failure, with 10% abrupt vessel closure (AVC), which Grüntzig had a tricky time explaining to seniors at his establishment, who had been lower than sympathetic, culminating with him leaving Zurich for Atlanta in 1980; getting into the US as a nationwide treasure.23 He was provided a professorship and limitless funding at Emory College, courtesy of a 100 million greenback grant from Coca Cola, which is headquartered at Atlanta.27 Grüntzig’s Lancet sequence describes 5 sufferers. One was a 44-year-old man with an undilatable calcified circumflex artery. One other man, Dölf Bachmann who was 38, coincidentally the identical age as Grüntzig on the time, was symptom free from his proximal left anterior descending (LAD) POBA for 23 years. He was additionally Grüntzig’s first coronary affected person handled on 16 September 1977.23 At 61 years of age, he had angina once more with borderline pressure-wire fractional circulate reserve of 0.84 and he had a bare-metal stent positioned, which failed inside two months. This was balloon dilated. He was properly for an additional 14 years till 75 years outdated when he had a DES for recurrent ISR. One may speculate that he would have had fewer repeat procedures if Bernhard Meier, Grüntzig’s protégé had entry to DCB. He detailed this man’s medical course in his Andreas Grüntzig Lecture on the thirty fifth European Society of Cardiology (ESC) Congress in London on 30 August 2015. Early adopters of POBA had a 6–10% failure price necessitating emergency CABG.25,28,29 There was a studying curve in case choice and skilful lesion preparation. As an illustration, Geoffrey Hartzler’s institutional failure price was below 1% after a decade’s follow, from 10%.28
Stent points
DES is advisable by pointers for STEMI.4 The CADILLAC (Managed Abciximab and Machine Investigation to Decrease Late Angioplasty Problems) research, which was carried out over 20 years in the past, seemingly confirmed the prevalence of stenting.30 However this was on the premise of deliberate target-vessel revascularisation at six months, which was not clinically pushed. However, expertise gained during the last twenty years has uncovered some downsides to stenting in STEMI. These embody no reflow from distal embolisation, inflicting microvascular obstruction that extends infarct measurement, as with side-branch occlusion.31,32 Within the mid-LAD, which is replete with aspect branches, the septal and diagonal branches are weak to occlude with stent optimisation from plaque or thrombotic shift. Conversely, stent mal-apposition may outcome from stent under-sizing from vasoconstriction throughout STEMI.33
With stenting basically, past 9 months there’s a steady threat of ISR, from 5–15% throughout the 12 months to a year-on-year rise to 25–30% in three to 5 years; this curve continues to climb, even with third-generation DES.20,34–37 The best stenting price might be round 30%, in keeping with Bernhard Meier, as per legislation of diminishing return for POBA and bare-metal stent.36 Conjecturally, the identical ratio holds true for DCB and DES. Goal-vessel failure may partly be pushed by vascular endothelial dysfunction that’s exacerbated by the stent.38 There may be additionally renewed curiosity within the coronary microvasculature.39 It performs a central position in coronary blood circulate autoregulation, which explains the disconnect between epicardial coronary artery illness, signs and mortality in sufferers with steady illness,40,41 power kidney illness (CKD),42 and coronary heart failure;43 the place DES imparts salutary and no lasting profit, nor does it affect survival within the unselected inhabitants.44
In one other Andreas Grüntzig Lecture on the forty second ESC Congress on 27 August 2022 in Barcelona, Javier Escaned cautioned {that a} third of every day coronary interventional follow now offers with stent failures. These are primarily attributable to the metallic stent strut and neo-atheroma. Neither thinner strut nor abluminal biodegradable polymer coating gives sturdy outcomes, and the seek for a bioresorbable stent stays elusive. Abbott’s Scaffold, a short-lived experiment with a bioresorbable poly-L-lactide strut, as a substitute gave rise to the imaging-guided stenting method. This includes in depth stenting for extra full plaque protection, probably contributing to additional stent failures, as stenting size of over 40 mm is a potent predictor.34,45
Plaque stabilisation?
The shortcomings of DES is perhaps prevented by DCB. The massive SCAAR (Swedish Coronary Angiography and Angioplasty Registry)46 and other47,48 analysis registries within the mode of post-marketing surveillance have demonstrated long-term efficacy and security of DCB in all-comers, together with STEMI. What’s exceptional is that the target-vessel failure curve flattens after three years, harking back to a ‘treatment’. That is additionally noticed in some randomised-controlled trials (RCTs) evaluating DES and DCB.5,49 Not not like that of POBA, within the creator’s 20-year follow, solely an 89-year-old lady re-presented for surveillance of her aortic stenosis. She had POBA 30 years prior in 1993 and has been angina free since. Maybe it is because, with out a stent-caged artery, POBA or DCB preserves vascular endothelial perform,50,51 regresses atherosclerotic plaque,52 and, in an animal experiment, stabilises weak plaque.53 The latter is being examined within the DEBuT-LRP (Intravascular Identification and Drug-Eluting Balloon Remedy of Susceptible Lipid-Wealthy Plaques) research (NCT04765956).
Abrupt vessel closure
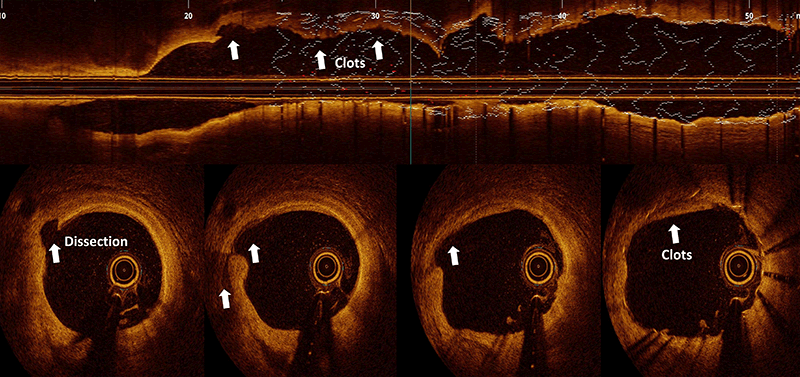
There may be undoubtedly a studying curve with DCB reminiscent of the POBA period.24,28 It’s clear that AVC is usually thrombotic,54 and infrequently is because of occlusive dissection.55 The previous is rare with trendy antiplatelet medicine pretreatment, whereas the latter requires stenting, and could possibly be anticipated with follow, such that it turns into much less frequent than acute stent thrombosis.1,55 In any other case, ambulatory DCB follow wouldn’t be possible.56 Strain-wire guided DCB,57 and managed plaque-modification,8 present added confidence. Though the worry of AVC with out stenting is actual, be that as it might, superior chronic-total occlusion (CTO) operators are fairly content material to go away a dissected vessel unstented as an funding process (Make investments CTO PCI Trial: NCT04774913). However, stent thrombosis happens in 0.8% (one in 125) and 1% of instances inside 30 days and one 12 months, respectively, in keeping with the BCIS nationwide audit knowledge. There are affected person and procedural elements. Technically, stent below enlargement and mal-apposition are most likely much less frequent with present follow, with the elevated consciousness for these, and the plethora of imaging and calcium modification units we now have in our armamentarium. Nevertheless, the reverse is perhaps occurring. Stent oversizing, aggressive post-dilatation or stenting right into a diseased phase causes stent-edge dissection (SED) in as much as 20% of instances, detectable with optical coherence tomography (OCT), which carries a 5% mortality inside three months.58 It’s because the ensuing flap of tissue past the distal stent edge goes towards the blood circulate, extending the dissection, impeding blood circulation and precipitating subacute stent thrombosis (determine 1).
POBA with out stenting could possibly be achieved in over 95% of STEMI instances in RCTs.10,30–32 Within the DANAMI-DEFER (Deferred versus Standard Stent Implantation in Sufferers with ST-segment Elevation Myocardial Infarction) research,31 deferring stenting for 3 days (612 stenting and 603 defer), AVC within the second half of research occurred in a single (<1%) case versus 11 (1.5%) instances indicating a learnable course of. Echocardiographic left ventricular ejection fraction was considerably higher within the defer group (60% vs. 57%, p=0.042). Within the Tremendous-MIMI (Minimalist Instant Mechanical Intervention) research,32 there was 1.2% AVC when stenting was delayed to at least one week, these instances didn’t obtain a glycoprotein IIb/IIIa inhibitor. Within the extra up-to-date EROSION III (Efficient Anti-Thrombotic Remedy With out Stenting: Intravascular Optical Coherence Tomography Primarily based Administration in Plaque Erosion) research,59 sufferers with plaque erosion on OCT had medical remedy in practically 60% of instances, suggesting that stenting is elective in STEMI. No AVC occurred, regardless of a 20% price of glycoprotein IIb/IIIa inhibitor use, in contrast with a 3rd within the DANAMI-DEFER research, however this research included a direct-acting third-generation P2Y12 inhibitor. STEMI AVC is, due to this fact, as predictable as in different settings.1,56,57 Importantly, intravascular imaging with OCT has highlighted the varied aetiologies of STEMI; plaque rupture, plaque erosion, calcium protrusion and an entire host of MINOCA (Myocardial Infarction with Non-Obstructive Coronary Artery) displays, the place stenting will not be advisable, corresponding to in spontaneous coronary artery dissection (SCAD) with spreading intramural haematoma, bridging phase, thrombotic or embolic occlusion, epicardial and microvascular vasospasm, and many others. STEMI intervention, therefore, could possibly be tailor-made and individualised. The STEMI pointers written in 2018 will have to be up to date.4
Hybrid provisional stenting technique
Stent use was largely off-label. The instruction to be used (IFU) of DES dictated one stent for an easy lesion. During which case, ISR, steel allergy, CTO, STEMI, lengthy lesion requiring two-stent overlap, vein graft, left foremost, bifurcation, ostial and three-vessel illness had been all handled on the operator’s discretion. Regardless of this, it drove technical innovation and refinement. The most effective attended classes at conferences are case opinions on unexpected challenges and get-out-of-trouble options, apparently labored out on the hoof. The center is a highly-sensitive life-sustaining organ reacting with immediacy to any invasive process. This permits the moment suggestions studying course of. Any complication arises self-evidently and if not immediate, could be inside a short while span. For instance, the double-barrel or simultaneous-kissing stenting for bifurcation lesion went out of favour swiftly due to early stent failure.60 As a substitute, crush stenting stays in use.61 Lim and Dzavik’s essential description of balloon crush of side-branch stent in 200462 permits for a stepwise method, giving rise to double-kiss (DK) crush stenting, which is the usual for two-stent technique.63 In Europe, single-stent method is favoured and, with DCB, it could possibly be hybrid provisional stenting for complicated bifurcation illness as illustrated in determine 2.
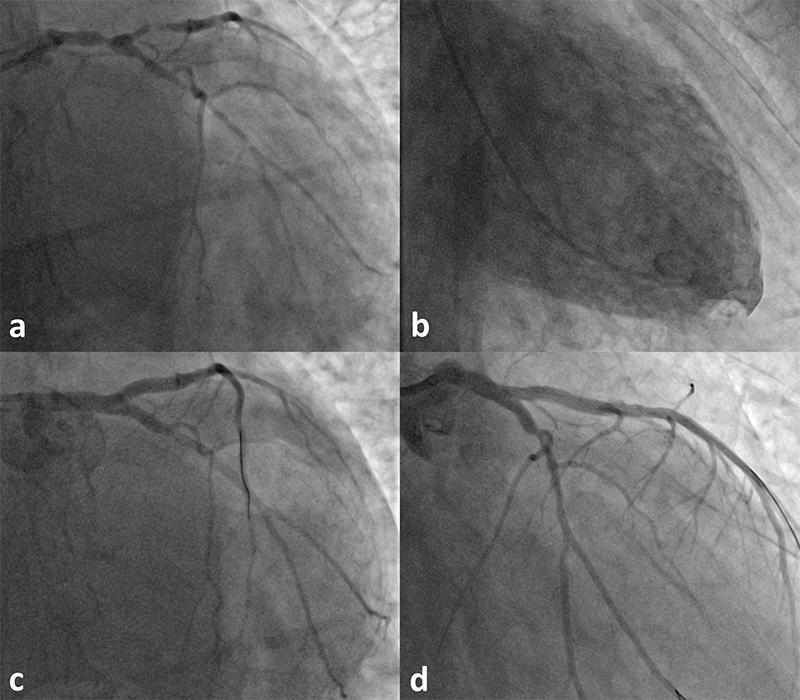
The hybrid provisional stenting technique limits stenting and permits underfilled and diseased vessel to rework, as demonstrated by Carlo Di Mario in a CTO case report.64 It’s being appraised in bifurcation RCTs.65,66 Any two-stent method creates stiff-and-thick multi-layered struts, mal-apposition and circulate turbulence within the neo-carina, as nidus for stent failure. In distinction, one-stent layer permits conformation to the artery lumen minimising ISR. Additional, T-stenting the aspect department first ensures its entry after main-branch stent trapping, the sliver of uncovered ostium is then handled with DCB. This system is fast, it permits simpler future re-intervention and it’s 5-French suitable, in addition to appropriate for the unstable affected person who tolerates myocardial ischaemia poorly.
Conclusion
It’s a good suggestion to heed many stent producers’ recommendation to limit to at least one non-overlapping DES if stenting is deliberate, in a straight phase, well-prepared and compliant if calcified, avoiding any bifurcation except it includes the left foremost coronary artery. The remaining is complemented with DCB, refraining from the spurious or purist argument of utilizing both DES or DCB. Use of DES with DCB directly simplifies and hastens coronary intervention. DCB is perhaps the first focus for STEMI sooner or later, as its various underlying mechanisms are thought of. AVC is rare with newer antiplatelet medicine, and is each preventable and predictable with follow. DES delays, moderately than prevents, target-vessel failure; from POBA that happens inside three to 5 months to 3 to 5 years and continues to fail in the end. With DCB the plaque seems to stabilise with plateauing occasion price. Lastly, DCB-alone technique carries no systematic penalty. For the stent fanatics, it could possibly be thought to be a defer-stent method, even when it fails it ends in restricted stenting in a bigger remodelled vessel, however stent deferment tends to be a long-term funding.
Key messages
Drug-coated balloon reduces coronary restenosis from plain-old-balloon-angioplasty, matching that of drug-eluting stent in de novo small vessel illness
It has been evaluated in the entire vary of coronary artery illness and its use is rising, particularly within the Far East
It causes luminal enlargement as a result of constructive vascular remodelling, preserves endothelial perform, probably stabilises the plaque and speculatively improves cardiac perform. Though its procedural end result, as with stenting, relies upon critically on lesion modification, i.e. ‘failure to organize is getting ready to fail’
Abrupt vessel closure after drug-coated balloon is preventable, predictable and is not any extra frequent than with stent thrombosis
When drug-coated balloon is used with drug-eluting stent it limits stenting and simplifies complicated coronary artery anatomy
Conflicts of curiosity
None declared.
Funding
None.
Affected person consent
The sufferers have kindly given their knowledgeable consent for his or her instances to be shared for discovered communication.
Acknowledgements
The creator skilled on the Toronto Normal Hospital (2003–2005) below Vladimir Dzavik. This began with the extreme acute respiratory syndrome (SARS CoV-1) outbreak, albeit on the tail finish. Procedures had been carried out with private safety gear as was the case with SARS CoV-2 or COVID-19 within the UK. Over the course of his fellowship, the prevailing philosophy of procedural success there, as was elsewhere, was outlined by stenting. Brachytherapy was employed for repeated bare-metal stent ISR and the first-generation DES use began to select up. Reviews of late-acquired stent mal-apposition and thrombosis emerged with post-marketing surveillance after two years, leading to Nationwide Institute for Well being and Care Excellence (NICE) pointers in 2008, which additionally took into consideration the prices; limiting second-generation DES to small vessel <3.0 mm in diameter and lesion >15 mm in size. Below this circumstance, the creator’s use of DES was <30% and the remaining had been bare-metal stent and POBA plus thrombectomy in STEMI. The creator’s first use of DCB was a DIOR in a 65-year-old man with CKD and proper coronary artery ISR on 10 December 2009. It failed inside six weeks. The second case was for a de novo ostial obtuse marginal department lesion in a 59-year-old man with steady angina on 11 January 2010 and he stays properly past 12 years. The creator attended Jim Nolan’s Transradial Masterclass in Manchester on 20–21 November 2014. Simon Eccleshall introduced an attention-grabbing de novo DCB case within the night angiographic evaluate session. The creator requested him which product he used. Alex Grimster (former head of physiology) put it on the cabinets inside six weeks. The creator participated in Simon Eccleshall’s DCB assembly in Birmingham on 4 September 2015 and the subsequent one on 29 September 2016 sharing his early DCB expertise. Within the following assembly on 28 September 2017, the creator introduced his LAD STEMI sequence and postulated on the stented LAD’s affect on cardiac perform. The creator thanks the medical seniors; Stephen Brecker, Rajan Sharma and Manav Sohal for his or her insightful and progressive management; additionally expresses gratitude to Mary Keal (Matron), Dinesh Sajnani (Head of Radiology), the sufferers handled by the creator together with the left foremost bifurcation case described on this manuscript, Klio Konstantinou and EnHui Yong (trainees) who assisted within the process, as illustrated on this report, and all of the cardiology employees who selflessly taken care of these sufferers. Lastly, this text is the creator’s private viewpoint written from his personal expertise, interpretation of literature and thru interactions with and listening to talks given by specialists within the discipline; Bruno Scheller, Franz Kleber, Klaus Bonaventura, Simon Eccleshall, Sandeep Basavarajaiah, Bernardo Cortese and Tuomas Rissanen.
References
1. Jeger RV, Eccleshall S, Wan Ahmad WA et al. Drug-coated balloons for coronary artery illness: third report of the Worldwide DCB Consensus Group. JACC Cardiovasc Interv 2020;13:1391–402. https://doi.org/10.1016/j.jcin.2020.02.043
2. Kleber FX, Schulz A, Waliszewski M et al. Native paclitaxel induces late lumen enlargement in coronary arteries after balloon angioplasty. Clin Res Cardiol 2015;104:217–25. https://doi.org/10.1007/s00392-014-0775-2
3. Scheller B, Speck U, Abramjuk C, Bernhardt U, Bohm M, Nickenig G. Paclitaxel balloon coating, a novel technique for prevention and remedy of restenosis. Circulation 2004;110:810–14. https://doi.org/10.1161/01.CIR.0000138929.71660.E0
4. Neumann FJ, Sousa-Uva M, Ahlsson A et al. 2018 ESC/EACTS pointers on myocardial revascularization. Eur Coronary heart J 2019;40:87–165. https://doi.org/10.1093/eurheartj/ehy855
5. Latib A, Ruparelia N, Menozzi A et al. 3-year follow-up of the Balloon Elution and Late Loss Optimization Examine (BELLO). JACC Cardiovasc Interv 2015;8:1132–4. https://doi.org/10.1016/j.jcin.2015.04.008
6. Jeger RV, Farah A, Ohlow MA et al. Drug-coated balloons for small coronary artery illness (BASKET-SMALL 2): an open-label randomised non-inferiority trial. Lancet 2018;392:849–56. https://doi.org/10.1016/S0140-6736(18)31719-7
7. Rissanen TT, Uskela S, Eranen J et al. Drug-coated balloon for remedy of de-novo coronary artery lesions in sufferers with excessive bleeding threat (DEBUT): a single-blind, randomised, non-inferiority trial. Lancet 2019;394:230–9. https://doi.org/10.1016/S0140-6736(19)31126-2
8. Chiew KLX, Lim PO. Three-year end result with drug-coated balloon percutaneous coronary intervention in coronary Takayasu arteritis: a case evaluate. Catheter Cardiovasc Interv 2021;97:841–6. https://doi.org/10.1002/ccd.29099
9. Li QY, Chang MY, Wang XY et al. Efficacy and security of drug-coated balloon within the remedy of acute myocardial infarction: a meta-analysis of randomized managed trials. Sci Rep 2022;12:6552. https://doi.org/10.1038/s41598-022-10124-z
10. Vos NS, Fagel ND, Amoroso G et al. Paclitaxel-coated balloon angioplasty versus drug-eluting stent in acute myocardial infarction: the REVELATION randomized trial. JACC Cardiovasc Interv 2019;12:1691–9. https://doi.org/10.1016/j.jcin.2019.04.016
11. Erdogan E, Li Z, Zhu YX et al. DCB mixed with provisional DES implantation within the remedy of De Novo Medina 0,1,0 or 0,0,1 left foremost coronary bifurcation lesions: a proof-of-concept research. Anatol J Cardiol 2022;26:218–25. https://doi.org/10.5152/AnatolJCardiol.2021.1157
12. Gunawardena TD, Corballis N, Merinopoulos I et al. Drug-coated balloon vs. drug-eluting stents for de novo unprotected left foremost stem illness: the SPARTAN-LMS research. J Cardiovasc Dev Dis 2023;10:84. https://doi.org/10.3390/jcdd10020084
13. Jiang ZM, Liu L. Drug-coated versus uncoated balloon for aspect department safety in coronary bifurcation lesions handled with provisional stenting utilizing drug-eluting stents: a meta-analysis. Int J Clin Pract 2022;2022:5892589. https://doi.org/10.1155/2022/5892589
14. Shin ES, Jun EJ, Kim S et al. Scientific affect of drug-coated balloon-based percutaneous coronary intervention in sufferers with multivessel coronary artery illness. JACC Cardiovasc Interv 2023;16:292–9. https://doi.org/10.1016/j.jcin.2022.10.049
15. Yu X, Wang X, Ji F et al. A non-inferiority, randomized medical trial evaluating paclitaxel-coated balloon versus new-generation drug-eluting stents on angiographic outcomes for coronary de novo lesions. Cardiovasc Medicine Ther 2022;36:655–64. https://doi.org/10.1007/s10557-021-07172-4
16. Aziz A, Bhatia G, Pitt M et al. Intravascular lithotripsy in calcified-coronary lesions: a real-world observational, European multicenter research. Catheter Cardiovasc Interv 2021;98:225–35. https://doi.org/10.1002/ccd.29263
17. Rissanen TT, Uskela S, Siljander A et al. Percutaneous coronary intervention of complicated calcified lesions with drug-coated balloon after rotational atherectomy. J Interv Cardiol 2017;30:139–46. https://doi.org/10.1111/joic.12366
18. Shiraishi J, Koshi N, Matsubara Y et al. Stent-less percutaneous coronary intervention utilizing rotational atherectomy and drug-coated balloon: a case sequence and a mini evaluate. Cardiovasc Revasc Med 2018;19:705–11. https://doi.org/10.1016/j.carrev.2018.02.007
19. Zheng B, Yi T, Wu Q, Bai F, Li J. Drug-coated balloon remedy for potential sequelae of Kawasaki illness evaluated by multi-modalities. Int Coronary heart J 2022;63:773–6. https://doi.org/10.1536/ihj.21-593
20. Volz S, Angeras O, Odenstedt J et al. Sustained threat of stent thrombosis and restenosis in first era drug-eluting stents after one decade of follow-up: a report from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). Catheter Cardiovasc Interv 2018;92:E403–E409. https://doi.org/10.1002/ccd.27655
21. Jolly SS, Yusuf S, Cairns J et al. Radial versus femoral entry for coronary angiography and intervention in sufferers with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet 2011;377:1409–20. https://doi.org/10.1016/S0140-6736(11)60404-2
22. Valgimigli M, Frigoli E, Leonardi S et al. Radial versus femoral entry and bivalirudin versus unfractionated heparin in invasively managed sufferers with acute coronary syndrome (MATRIX): closing 1-year outcomes of a multicentre, randomised managed trial. Lancet 2018;392:835–48. https://doi.org/10.1016/S0140-6736(18)31714-8
23. Meier B, Bachmann D, Luscher T. 25 years of coronary angioplasty: nearly a fairy story. Lancet 2003;361:527. https://doi.org/10.1016/S0140-6736(03)12470-1
24. Grüntzig A. Transluminal dilatation of coronary-artery stenosis. Lancet 1978;311:263. https://doi.org/10.1016/S0140-6736(78)90500-7
25. Barton M, Grüntzig J, Husmann M, Rosch J. Balloon angioplasty – the legacy of Andreas Grüntzig, M.D. (1939–1985). Entrance Cardiovasc Med 2014;1:15. https://doi.org/10.3389/fcvm.2014.00015
26. Anderson HVS. Andreas R. Gruentzig, MD (1939–1985). Cardiology 2022;147:107–12. https://doi.org/10.1159/000519303
27. Meier B. His grasp’s artwork, Andreas Grüntzig’s method to performing and educating coronary angioplasty. EuroIntervention 2017;13:15–27. https://doi.org/10.4244/EIJV13I1A2
28. Hartzler GO. PTCA in evolution: why is it so well-liked? Cleve Clin J Med 1990;57:121–4. https://doi.org/10.3949/ccjm.57.2.121
29. Sowtgon E, de Bono D, Gribbin B, Man FS, Silverton P. Coronary angioplasty in the UK. Report of a Working Occasion of the British Cardiac Society. Br Coronary heart J 1991;66:325–31. https://doi.org/10.1136/hrt.66.4.325
30. Stone GW, Grines CL, Cox DA et al. Comparability of angioplasty with stenting, with or with out abciximab, in acute myocardial infarction. N Engl J Med 2002;346:957–66. https://doi.org/10.1056/NEJMoa013404
31. Kelbaek H, Hofsten DE, Kober L et al. Deferred versus standard stent implantation in sufferers with ST-segment elevation myocardial infarction (DANAMI 3-DEFER): an open-label, randomised managed trial. Lancet 2016;387:2199–206. https://doi.org/10.1016/S0140-6736(16)30072-1
32. Mester P, Bouvaist H, Delarche N et al. At the very least seven days delayed stenting utilizing minimalist fast mechanical intervention (MIMI) in ST-segment elevation myocardial infarction: the SUPER-MIMI research. EuroIntervention 2017;13:390–6. https://doi.org/10.4244/EIJ-D-16-00667
33. Adriaenssens T, Joner M, Godschalk TC et al. Optical coherence tomography findings in sufferers with coronary stent thrombosis: a report of the PRESTIGE Consortium (Prevention of Late Stent Thrombosis by an Interdisciplinary International European Effort). Circulation 2017;136:1007–21. https://doi.org/10.1161/CIRCULATIONAHA.117.026788
34. Kong MG, Han JK, Kang JH et al. Scientific outcomes of lengthy stenting within the drug-eluting stent period: patient-level pooled evaluation from the GRAND-DES registry. EuroIntervention 2021;16:1318–25. https://doi.org/10.4244/EIJ-D-19-00296
35. Kereiakes DJ, Windecker S, Jobe RL et al. Scientific outcomes following implantation of thin-strut, bioabsorbable polymer-coated, everolimus-eluting SYNERGY stents. Circ Cardiovasc Interv 2019;12:e008152. https://doi.org/10.1161/CIRCINTERVENTIONS.119.008152
36. Brophy JM, Belisle P, Joseph L. Proof to be used of coronary stents. A hierarchical bayesian meta-analysis. Ann Intern Med 2003;138:777–86. https://doi.org/10.7326/0003-4819-138-10-200305200-00005
37. Brodie BR, Pokharel Y, Garg A et al. Very late hazard with stenting versus balloon angioplasty for ST-elevation myocardial infarction: a 16-year single-center expertise. J Interv Cardiol 2014;27:21–8. https://doi.org/10.1111/joic.12082
38. Lim PO. Angina with coronary microvascular dysfunction and its physiological evaluation: a evaluate with instances. Br J Cardiol 2022;29:13. https://doi.org/10.5837/bjc.2022.013
39. Boden WE, Marzilli M, Crea F et al. Evolving administration paradigm for steady ischemic coronary heart illness sufferers: JACC evaluate matter of the week. J Am Coll Cardiol 2023;81:505–14. https://doi.org/10.1016/j.jacc.2022.08.814
40. Al-Lamee R, Thompson D, Dehbi HM et al. Percutaneous coronary intervention in steady angina (ORBITA): a double-blind, randomised managed trial. Lancet 2018;391:31–40. https://doi.org/10.1016/S0140-6736(17)32714-9
41. Maron DJ, Hochman JS, Reynolds HR et al. Preliminary invasive or conservative technique for steady coronary illness. N Engl J Med 2020;382:1395–407. https://doi.org/10.1056/NEJMoa1915922
42. Herzog CA, Simegn MA, Xu Y et al. Kidney transplant listing standing and outcomes within the ISCHEMIA-CKD trial. J Am Coll Cardiol 2021;78:348–61. https://doi.org/10.1016/j.jacc.2021.05.001
43. Perera D, Clayton T, O’Kane PD et al. Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med 2022;387:1351–60. https://doi.org/10.1056/NEJMoa2206606
44. Coughlan JJ, Raber L, Brugaletta S et al. Intercourse variations in 10-year outcomes after percutaneous coronary intervention with drug-eluting stents: insights from the DECADE cooperation. Circulation 2023;147:575–85. https://doi.org/10.1161/CIRCULATIONAHA.122.062049
45. Onuma Y, Chevalier B, Ono M et al. Bioresorbable scaffolds versus everolimus-eluting metallic stents: five-year medical outcomes of the randomised ABSORB II trial. EuroIntervention 2020;16:e938–e941. https://doi.org/10.4244/EIJ-D-20-00024
46. Venetsanos D, Omerovic E, Sarno G et al. Long run end result after remedy of de novo coronary artery lesions utilizing three completely different drug coated balloons. Int J Cardiol 2021;325:30–6. https://doi.org/10.1016/j.ijcard.2020.09.054
47. Lee SY, Cho YK, Kim SW et al. Scientific outcomes of drug-coated balloon remedy in a large-scale multicenter Korean registry research. Korean Circ J 2022;52:444–54. https://doi.org/10.4070/kcj.2021.0261
48. Merinopoulos I, Gunawardena T, Wickramarachchi U et al. Lengthy-term security of paclitaxel drug-coated balloon-only angioplasty for de novo coronary artery illness: the SPARTAN DCB research. Clin Res Cardiol 2021;110:220–7. https://doi.org/10.1007/s00392-020-01734-6
49. Scheller B, Vukadinovic D, Jeger R et al. Survival after coronary revascularization with paclitaxel-coated balloons. J Am Coll Cardiol 2020;75:1017–28. https://doi.org/10.1016/j.jacc.2019.11.065
50. Kawai T, Watanabe T, Yamada T et al. Coronary vasomotion after remedy with drug-coated balloons or drug-eluting stents: a potential, open-label, single-centre randomised trial. EuroIntervention 2022;18:e140–e148. https://doi.org/10.4244/EIJ-D-21-00636
51. Kim S, Lee JS, Kim YH et al. Favorable vasomotor perform after drug-coated balloon-only angioplasty of de novo native coronary artery lesions. J Clin Med 2022;11:299. https://doi.org/10.3390/jcm11020299
52. Yamamoto T, Sawada T, Uzu Okay, Takaya T, Kawai H, Yasaka Y. Attainable mechanism of late lumen enlargement after remedy for de novo coronary lesions with drug-coated balloon. Int J Cardiol 2020;321:30–7. https://doi.org/10.1016/j.ijcard.2020.07.028
53. Chowdhury MM, Singh Okay, Albaghdadi MS et al. Paclitaxel drug-coated balloon angioplasty suppresses development and irritation of experimental atherosclerosis in rabbits. JACC Primary Transl Sci 2020;5:685–95. https://doi.org/10.1016/j.jacbts.2020.04.007
54. Rothberg MB, Celestin C, Fiore LD, Lawler E, Prepare dinner JR. Warfarin plus aspirin after myocardial infarction or the acute coronary syndrome: meta-analysis with estimates of threat and profit. Ann Intern Med 2005;143:241–50. https://doi.org/10.7326/0003-4819-143-4-200508160-00005
55. Huber MS, Mooney JF, Madison J, Mooney MR. Use of a morphologic classification to foretell medical end result after dissection from coronary angioplasty. Am J Cardiol 1991;68:467–71. https://doi.org/10.1016/0002-9149(91)90780-O
56. Merinopoulos I, Wickramarachchi U, Wardley J et al. Day case discharge of sufferers handled with drug coated balloon solely angioplasty for de novo coronary artery illness: a single heart expertise. Catheter Cardiovasc Interv 2020;95:105–08. https://doi.org/10.1002/ccd.28217
57. Shin ES, Ann SH, Balbir Singh G, Lim KH, Kleber FX, Koo BK. Fractional circulate reserve-guided paclitaxel-coated balloon remedy for de novo coronary lesions. Catheter Cardiovasc Interv 2016;88:193–200. https://doi.org/10.1002/ccd.26257
58. Jinnouchi H, Sakakura Okay, Yanase T et al. Influence of stent edge dissection detected by optical coherence tomography after current-generation drug-eluting stent implantation. PLoS One 2021;16:e0259693. https://doi.org/10.1371/journal.pone.0259693
59. Jia H, Dai J, He L et al. EROSION III: a multicenter RCT of OCT-guided reperfusion in STEMI with early infarct artery patency. JACC Cardiovasc Interv 2022;15:846–56. https://doi.org/10.1016/j.jcin.2022.01.298
60. Morris PD, Iqbal J, Chiastra C, Wu W, Migliavacca F, Gunn JP. Simultaneous kissing stents to deal with unprotected left foremost stem coronary artery bifurcation illness; stent enlargement, vessel harm, hemodynamics, tissue therapeutic, restenosis, and repeat revascularization. Catheter Cardiovasc Interv 2018;92:E381–E392. https://doi.org/10.1002/ccd.27640
61. Raphael CE, O’Kane PD, Johnson TW et al. Evolution of the crush method for bifurcation stenting. JACC Cardiovasc Interv 2021;14:2315–26. https://doi.org/10.1016/j.jcin.2021.08.048
62. Lim PO, Dzavik V. Balloon crush: remedy of bifurcation lesions utilizing the crush stenting method as tailored for transradial method of percutaneous coronary intervention. Catheter Cardiovasc Interv 2004;63:412–16. https://doi.org/10.1002/ccd.20179
63. Chen X, Li X, Zhang JJ et al. 3-year outcomes of the DKCRUSH-V trial evaluating DK crush with provisional stenting for left foremost bifurcation lesions. JACC Cardiovasc Interv 2019;12:1927–37. https://doi.org/10.1016/j.jcin.2019.04.056
64. Ciardetti N, Nardi G, Di Mario C. Direct high-frequency intravascular ultrasound visualization of drug supply after paclitaxel urea eluting balloon angioplasty. Eur Coronary heart J 2023;44:1096. https://doi.org/10.1093/eurheartj/ehad020
65. Gao XF, Ge Z, Kan J et al. Rationale and design for comparability of non-compliant balloon with drug-coating balloon angioplasty for aspect department after provisional stenting for sufferers with true coronary bifurcation lesions: a potential, multicentre and randomised DCB-BIF trial. BMJ Open 2022;12:e052788. https://doi.org/10.1136/bmjopen-2021-052788
66. Guo Q, Peng L, Rao L et al. The “L-Sandwich” technique for true coronary bifurcation lesions: a randomized medical trial. J Interv Cardiol 2023;2023:6889836. https://doi.org/10.1155/2023/6889836










{kind=link}